Most patients who come to the hospital after a DVT diagnosis have already spent two frightening hours reading things online that made them feel worse, not better. This article is my attempt to fix that — written from ten years of managing DVT in Delhi, in the words I use when I sit across from a patient and their family on the first day.
The call or the report that says deep vein thrombosis is frightening. It is supposed to be taken seriously — but it is not supposed to be a death sentence, and in the vast majority of cases, it is not. What matters more than the diagnosis itself is what you do in the next 48 hours, and who you speak to. As someone who has treated hundreds of DVT cases as a DVT Specialist in Delhi — including cases that other facilities had given up on — I want to walk you through this clearly, step by step.
First: What Is Actually Happening in Your Leg?
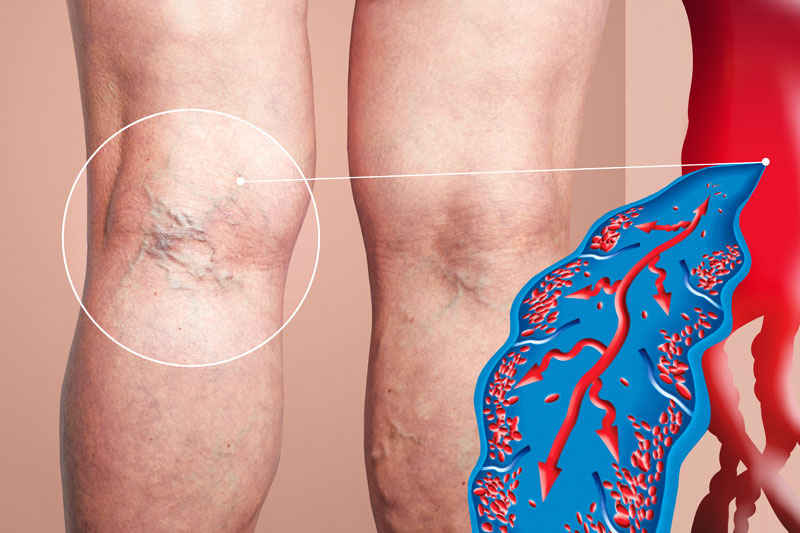
A blood clot in your deep leg vein — typically the popliteal vein behind the knee, the femoral vein in the thigh, or the iliac vein in the pelvis — is blocking normal venous blood flow. Your leg feels swollen, heavy, and warm because blood is backing up behind the blockage. The skin may feel tight and tender to the touch. These are not signs of the clot “moving” — they are signs of venous congestion, which is painful but not immediately dangerous.
The actual danger is different: a portion of the clot can detach, travel through the venous system, pass through the heart, and lodge in the pulmonary arteries — the vessels supplying your lungs. This is a pulmonary embolism, and large ones can be fatal within minutes. This is why DVT is always treated as urgent, even when the patient feels relatively well. The leg symptoms and the pulmonary risk are two separate things, and both need to be assessed simultaneously.
When a patient walks in with a swollen leg, my first question is never ‘how long has this been swollen?’ — it is ‘are you breathing normally right now?’ Pulmonary embolism can be silent until it is catastrophic. We rule it out first.
The First 24 Hours: What Assessment Looks Like
When you come in for evaluation of a suspected DVT, the first tool is a duplex ultrasound — an ultrasound that images the vein structure and also measures blood flow direction and speed. It is non-invasive, takes about 20 to 30 minutes, and is remarkably accurate for clots in the leg veins. If the clot is suspected to extend into the pelvis or abdomen — areas that ultrasound cannot see well through tissue — a CT venography or MRI may follow.
Simultaneously, a D-dimer blood test may be ordered. Elevated D-dimer alone does not confirm DVT, but a negative result in a low-risk patient can effectively rule it out, avoiding unnecessary imaging. Blood tests will also assess kidney function (relevant for contrast imaging), clotting factors, and in younger patients or those with no obvious trigger, a full thrombophilia screen — testing for inherited clotting disorders like Factor V Leiden, Protein C or S deficiency, and antiphospholipid antibodies.
In parallel, a CT pulmonary angiography (CTPA) is ordered if there are any respiratory symptoms — shortness of breath, chest pain, rapid heart rate, or drop in oxygen levels. Many patients with large DVTs have small, clinically silent pulmonary emboli that are found on imaging. Finding them changes the treatment approach significantly.
Treatment Is Not One-Size-Fits-All — Here Is How We Decide
This is the part that most online articles get wrong by oversimplifying. DVT treatment is highly individualised. The decision tree I walk through mentally for every patient includes: Where is the clot? How extensive is it? How long has it been there? What are the patient’s bleeding risks? What is their kidney function? Do they have cancer, pregnancy, recent surgery, or an underlying thrombophilia? Is this a first DVT or a recurrence?
Option 1 — Anticoagulation (Blood Thinners)
For the majority of below-knee and uncomplicated above-knee DVTs that are caught relatively early and where the patient has no major pulmonary involvement, anticoagulation is the starting treatment. Modern oral anticoagulants — specifically the DOACs (Direct Oral Anticoagulants) like rivaroxaban or apixaban — have simplified treatment enormously. They work fast, require no injections, and in most cases need no regular blood monitoring. Treatment duration is typically three to six months for a first provoked DVT (one with a clear trigger like surgery or immobilisation), and potentially indefinite for unprovoked recurrent DVTs.
Anticoagulation does not dissolve the clot. It prevents the existing clot from growing and prevents new clots from forming, while the body’s own fibrinolytic system gradually breaks down the existing thrombus over weeks to months. The risk of anticoagulation is bleeding — which is why it requires careful assessment of each individual’s baseline bleeding risk before starting.
Option 2 — Catheter-Directed Thrombolysis (CDT)
For more extensive clots — particularly those involving the iliac veins or the iliac-femoral segment — anticoagulation alone may leave the patient with significant residual clot burden, increasing the risk of post-thrombotic syndrome (PTS): a chronic condition causing persistent leg swelling, skin changes, and venous ulcers that can be debilitating. In these cases, catheter-directed thrombolysis is considered. A thin catheter is threaded directly into the clot under imaging guidance, and a clot-dissolving drug (tPA) is infused directly at the site of the blockage over 12 to 24 hours. This is far more effective and safer than giving systemic thrombolytics through a vein in the arm, because the dose is targeted and much lower.
Option 3 — Mechanical Clot Suction for DVT
This is where we are seeing the most exciting progress in vascular medicine, and it is an area where my practice in Delhi has invested significantly. Mechanical thrombectomy — what patients often call clot suction for DVT — uses catheter-based devices to physically remove the clot in a single session, without the bleeding risks of thrombolytic drugs.
Two systems I use routinely are the Angiojet system and the Penumbra CAT 16 lightning device. The Angiojet uses high-velocity saline jets to break up the clot and simultaneously suction it out — a process called rheolytic thrombectomy. The Penumbra device uses a large-bore aspiration catheter to vacuum out the clot directly. The Inari FlowTriever system, developed specifically for DVT, uses a mechanical retrieval mechanism to extract clot en masse from the iliac and femoral veins.
The advantage is speed. Instead of leaving a catheter in place for 24 hours infusing drugs, a mechanical thrombectomy can open the vessel in a single 60 to 90 minute procedure done under local anaesthesia with light sedation. Patients typically go home the next day. This makes it particularly valuable for patients with phlegmasia — a severe form of DVT where the clot load is so extensive that limb viability is at risk — or for patients who cannot receive thrombolytics due to bleeding risk. This is what distinguishes accessing the best DVT Treatment In Delhi from a standard hospital setting: not all centres in Delhi have these devices or the training to use them optimally.
Option 4 — IVC Filter Placement
In patients where anticoagulation is absolutely contraindicated — active bleeding, recent brain surgery, pregnancy in certain stages — and where the DVT clot burden is high, a retrievable IVC (inferior vena cava) filter can be placed as a temporary mechanical barrier. This small, umbrella-like device sits inside the body’s largest vein and catches any clot fragments before they can reach the lungs. It is a bridge strategy — once anticoagulation becomes safe, the filter is retrieved through the same catheter-based approach it was placed with.
The Question Most Patients Ask That No One Answers: Will My Leg Go Back to Normal?
Honestly — it depends on three things: how much clot was there, how quickly it was treated, and how well the deep venous valves survived. DVT damages the valves inside the veins that prevent blood from refluxing backward. When these valves are destroyed by the clot or by the inflammation from the clot, post-thrombotic syndrome can develop even after the clot is gone.
Patients who receive mechanical thrombectomy or CDT early — within 14 days of clot formation — have significantly better valve preservation and significantly lower rates of post-thrombotic syndrome compared to those treated with anticoagulation alone. This is not a minor quality-of-life issue: PTS can mean a permanently swollen, painful leg that requires lifelong compression stockings and recurrent ulcer management. It is one of the strongest arguments for pursuing aggressive endovascular treatment when the patient is a candidate.
If you want a complete view of what recovering from a DVT looks like in real patients — including before and after imaging — the vascular surgery gallery on our website documents many of these cases with clinical context.
When to Be Concerned About DVT — Even Without a Diagnosis Yet
Seek evaluation immediately if you experience any of the following: sudden swelling in one leg that was not there yesterday; warmth and redness in the calf or thigh; pain in the leg that worsens when you flex the foot upward; a history of recent surgery, cancer, long-haul flight, or extended bed rest; or any combination of leg symptoms with chest pain, shortness of breath, or rapid heartbeat. Do not take a “wait and see” approach. DVT is one of the few vascular emergencies where a 24-hour delay can mean the difference between a straightforward outpatient treatment and an ICU admission for pulmonary embolism.
You can read through more frequently asked questions about clots, vascular conditions, and what to expect from treatment at the vascular surgery FAQs page, which I have built specifically to address the questions patients are too afraid to ask in a consultation room.
Why the Specialist You Choose for DVT Matters More Than the Hospital Name
Delhi has excellent hospital infrastructure — but not all hospitals have a dedicated, subspecialty-trained Vascular Surgeon In Delhi who handles DVT as a primary focus. DVT is frequently managed by general physicians, cardiologists, or general surgeons who may not have access to — or training in — mechanical thrombectomy devices. The result is over-reliance on anticoagulation alone, which is appropriate for mild disease but suboptimal for the iliofemoral DVTs that carry the highest risk of long-term disability.
When choosing your Best DVT Treatment Doctor In Delhi, ask specifically: Do you perform mechanical thrombectomy? Which devices do you have access to? How many iliofemoral DVT interventions do you perform per year? What is your approach to post-thrombotic syndrome prevention? These questions cut through the marketing and tell you immediately whether you are speaking to someone who will give you a customised, evidence-driven treatment plan — or someone who will start you on a blood thinner and follow up in three months.
What Happens After Treatment: Living With (and Past) DVT
Recovery from DVT is active, not passive. During the anticoagulation period, you will need regular follow-up to monitor for recurrence, assess residual clot burden, and adjust treatment duration based on ongoing risk factors. Compression stockings — medical-grade, fitted, knee-high or thigh-high — are recommended for at least two years after proximal DVT to reduce the risk of post-thrombotic syndrome, regardless of whether you had anticoagulation alone or an interventional procedure.
Lifestyle factors matter. Maintaining a healthy weight, staying hydrated, avoiding prolonged immobilisation, and wearing compression during long flights all reduce recurrence risk. For patients with an inherited thrombophilia or unprovoked DVT, lifelong anticoagulation may be recommended — a decision made carefully after weighing bleeding risk against clot recurrence risk.
DVT, when managed correctly by the right Best Vascular Surgeon In New Delhi, is a condition most patients move fully past. The key is acting early, choosing a specialist rather than a generalist, and not settling for a treatment plan that was not designed specifically for your clot, your anatomy, and your life circumstances.
If you are dealing with a new DVT diagnosis — or you are worried your existing treatment is not working — I encourage you to reach out directly. A second opinion in vascular medicine is never wasted time. You can contact us through the contact page or visit bestvascularsurgeondelhi.com to learn more about the full scope of vascular care available in Delhi. You can also explore more about the complete team and philosophy at the about page.